Pay Type
: Credit(AROGYA SREE)
Age/Gender
: 48 Years/Female
Discharge Type: Relieved
Admission Date: 19/04/2024 09:30 PM
Diagnosis
SEPTIC SHOCK WITH MULTIPLE ORGAN DYSFUNCTION (RESOLVED) SECONDARY TO LEFT DIABETIC FOOT
S/P: DISARTICULATION OF LEFT GREAT TOE(13/04/2024) K/C/O TYPE 2 DIABETES MELLITUS SINCE 6 YEARS
1 PRBC TRANSFUSION DONE
Case History and Clinical Findings
CHIEF COMPLAINTS:
WOUND OVER THE LEFT FOOT SINCE 4 MONTHS
HISTORY OF PRESENT ILLNESS:
PATIENT WAS APPARENTLY ASYMPTOMATIC 4 MONTHS BACK, AFTER WHICH SHE DEVELOPED BLACKISH DISCOLORATION OF LEFT GREAT TOE WHICH WAS INSIDIOUS IN ONSET ,GRADUALLY PROGRESSIVE , ASSOCIATED WITH SWELLING OF THE INVOLVED LIMB TILL MID FOOT FOR WHICH SHE WENT TO A LOCAL RMP AND WAS TREATED WITH DRESSING .THERE WAS NO IMPROVEMENT, WITH PROGRESSION OF WOUND , ASSOCIATED WITH FOUL SMELLING DISCHARGE FOR WHICH SHE WAS TAKEN TO AN OUTSIDE HOSPITAL WHERE DISARTICULATON OF LEFT GREAT TOE WAS DONE UNDER REGIONAL ANESTHESIA ON 13/04/24.
CAME ON LAMA TO OUR HOSPITAL FOR FURTHER MANAGEMENT NO H/O FEVER,COUGH,COLD.
NO H/O CHEST PAIN,PALPITATIONS,BREATHLESSNESS,ORTHOPNEA,PND. NO H/O ABDOMINAL PAIN,BURNING MICTURITION,NAUSEA,VOMITING.
HISTORY OF PAST ILLNESS:
K/C/O TYPE 2 DIABETES MELLITUS SINCE 6 YEARS (ON TAB GLIMI M1/OD) NO H/O HYPERTENSION,ASTHMA,TB,EPILEPSY,CVA,CAD,CKD,CLD.
TREATMENT HISTORY:
ON TAB.GLIMI-M1 PO/OD
PERSONAL HISTORY:
MARRIED OCCUPATION: FARMER APPETITE: NORMAL DIET: MIXED
BOWEL AND BLADDER: REGULAR KNOWN ALLERGIES: NO ADDICTIONS: NO
FAMILY HISTORY:
NO SIGNIFICANT HISTORY.
GENERAL EXAMINATION :
PT IS CONCIOUS , COHERENT AND COOPERATIVE , MODERATLY BUILT AND NOURISHED . PALLOR PRSENT.
NO ICTERUS , CYANOSIS, CLUBBING ,LYMPHADENOPATHY, EDEMA. TEMP - 97.6 F
PR- 86 BPM
RR- 18 CPM
BP- 80/50 MMHG SPO2- 98% AT RA
GRBS- 164 MG/DL
SYSTEMIC EXAMINATION :
CVS - S1,S2 HEARD , NO MURMURS
RS - VESICULAR BREATH SOUNDS HEARD , NO WHEEZE AND DYSPNEA,NO CREPTS P/A- SOFT , NON-TENDER , NO ORGANOMEGALY
CNS -
LEVEL OF CONCIOUSNESS: CONCIOUS SPEECH: INCOHERENT
SIGNS OF MENINGEAL IRRITATION: NEGATIVE CRANIAL NERVES: NAD
MOTOR SYSTEM:
L R
TONE:UL- NORMAL NORMAL LL- NORMAL NORMAL POWER: 5/5 5/5
GLASGOW SCALE: E4V5M6 REFLEXES:
L R
BICEPS 2+ 2+
TRICEPS 2+ 2+ SUPINATOR + + KNEE 2+ 2+
ANKLE NOT ELICITABLE + PLANTARS- FLEXOR
COURSE IN THE HOSPITAL :
48 YEAR OLD FEMALE CAME TO CASUALITY WITH CHIEF COMPLAINTS OF WOUND ON LEFT FOOT SINCE 4 MONTH.
PATIENT WAS APPARENTLY ASYMPTOMATIC 4 MONTHS AGO THEN SHE DEVELOPED BLACKISH DISCOLORATION OF LEFT GREAT TOE SINCE 4 MONTHS,INSIDIOUS IN ONSET,GRADUALLY PROGRESSIVE ASSOCIATED WITH SWELLING OF LEFT FOOT.
PATIENT INITIALLY WENT TO OUTSIDE HOSPITAL IN HYDERABAD AND GOT DISARTICULATION OF LEFT GREAT TOE ON 13/04/2024 AND WAS ON IONOTROPIC SUPPORT AND WAS MANAGED THERE FOR 4-5 DAYS AND THEY GOT LAMA DISCHARGE FROM HOSPITAL DUE TO PERSONAL REASONS.
AS PATIENT CAME WITH FOLEYS IN SITU, FOLEYS WAS CHANGED ON THE DAY 1 OF ADMISSION AND DECATHETERISED ON DAY 5 OF ADMISSION.
ON ARRIVAL PATIENT BP-90/50 MMHG WITH NORAD 4 ML/HR GRBS- 165 MG/DL ON INJ. INSULIN HAI SC/TID.
PATIENT WAS ADMITTED IN ICU AND WAS STARTED ON INJ. HAI SC/TID AND INJ. NPH BD ACCORDING TO RBS LEVELS.
IONOTROPES INJ. NORADRENALINE AND INJ. VASOPRESSIN INFUSIONS STARTED AND TITRATED ACCORDINGLY TO MAINTAIN MAP(MEAN ARTERIAL PRESSURE) >65 MMHG. PATIENT TREATED WITH BROAD SPECTRUM ANTIBIOTICS. NECESSARY INVESTIGATIONS
WERE DONE AND BLOOD,URINE CULTURE AND SENSTIVITY SAMPLES SENT AND OTHER
NECESSARY INVESTIGATIONS WERE DONE.PATIENT WAS STARTED ON DUAL IONOTROPES AND ,RIGHT IJV TRIPLE LUMEN CATHETERISATION WAS DONE 21/04/24 UNDER ASEPTIC CONDITIONS AND THE PROCEDURE WAS UNEVENTFUL; WOUND DRESSINGS WERE DONE ON REGULAR BASIS,AFTER CROSS CONSULTATION WITH GENERAL SURGERY .
GENERAL SURGERY ON 19/04/24 I/V/O DIABETIC ULCER OVER LEFT FOOT:
HIGH PROTEIN DIET. (DIABETIC PROTEIN POWDER 2 TBSP IN GLASS OF MILK PO/BD)
T.CHYMEROL FORTE PO/TID.
BOTH LOWER LIMB ELEVATION.
REGULAR ASD( MGSO4 DRESSING FOR LEFT LOWER LIMB).
IONOTROPIC SUPPORT WAS STOPPED ON 23/4/2024 AND PATIENT IS HEMODYNAMICALLY STABLE.
BLOOD TRANSFUSION (1 UNIT PRBC) DONE ON 25/04/2024 I/V/O HEMOGLOBIN - 7.6G/DL
.POST TRANSFUSION Hb 10.2 G/DL.
GENERAL SURGERY REFERRAL WAS DONE ON 24/04/24 I/V/O DIABETIC ULCER OVER LEFT FOOT:
DEBRIDEMENT OF ULCER AND PAPAYA DRESSING DONE.
DURING THE STAY IN THE HOSPITAL , PATIENT WAS ACTIVELY AMBULATED . FROM DAY 4 OF ADMISSION HEALTHY GRANULATION TISSUE WAS FORMED IN THE WOUND.
PATIENT IS BEING DISCHARGED AS SHE SHOWED SIGNS OF PROGRESSIVE HEALING AND IS HEMODYNAMICALLY STABLE, WITH GLYCEMIC CONTROL.
Investigation
HBsAg-RAPID 19-04-2024 10:26:PM Negative
Anti HCV Antibodies - RAPID 19-04-2024 10:26:PM Non Reactive HIV 1/2 RAPID TEST: NON REACTIVE
URINE FOR CULTURE AND SENSTIVITY:
1-2 PUS CELLS SEEN.
PLENTY OF BUDDING YEAST CELLS SEEN.
NON ALBICANS CANDIDA >10* CFU/ML OF URINE.
SWAB FOR CULTURE AND SENSTIVITY:
FEW PUS CELLS,OCCASIONAL GRAM POSITIVE COCCI IN SINGLES SEEN,OCCASIONAL GRAM NEGATIVE BACILLI SEEN.
NON ALBICANS CANDIDA ISOLATED.
BLOODFOR CULTURE AND SENSTIVITY:
NO GROWTH AFTER 48 HOURS OF AEROBIC INCUBATION.
USG ABDOMEN DONE ON 20/04/2024:
LIVER- NORMAL S/E,NO F/L PV-NORMAL,NO IHBRD CBD- NORMAL
GALL BLADDER- DISTENDED;WALL THICKNESS- NORMAL PANCREAS- HEAD VISUALISED,NORMAL S/E
SPLEEN- 9.2 CM NORMAL S/E
RIGHT KIDNEY- 9.9 X 4.1 CM,NORMAL S/INCREASED ECHOGENICITY,CMD+ LEFT KIDNEY- 8.4 X 3.7 CM,NORMAL S/INCREASED ECHOGENICITY,CMD+ AORTA I.V.C. - NORMAL
NO ASCITES
NO LYMPHADENOPATHY
U.BLADDER- EMPTY,FOLEYS CATHETER INSERTED. PELVIS COULD NOT BE ASSESSED.
IMPRESSION:
-RAISED ECHOGENICITY OF BILATERAL KIDNEYS.
2-D ECHO DONE ON 23/04/2024:
NO RWMA.
TRIVIAL TR+/AR+/MR+.
MAC+ ; SCLEROTIC AV ; NO AS/MS.
- EF=59% ; RVSP=23+10=33MMHG.
GOOD LV SYSTOLIC FUNCTION.
GRADE 1 DIASTOLIC DYSFUNCTION+.
MINIMAL PE+.
IVC SIZE (0.8 CMS) COLLAPSING.
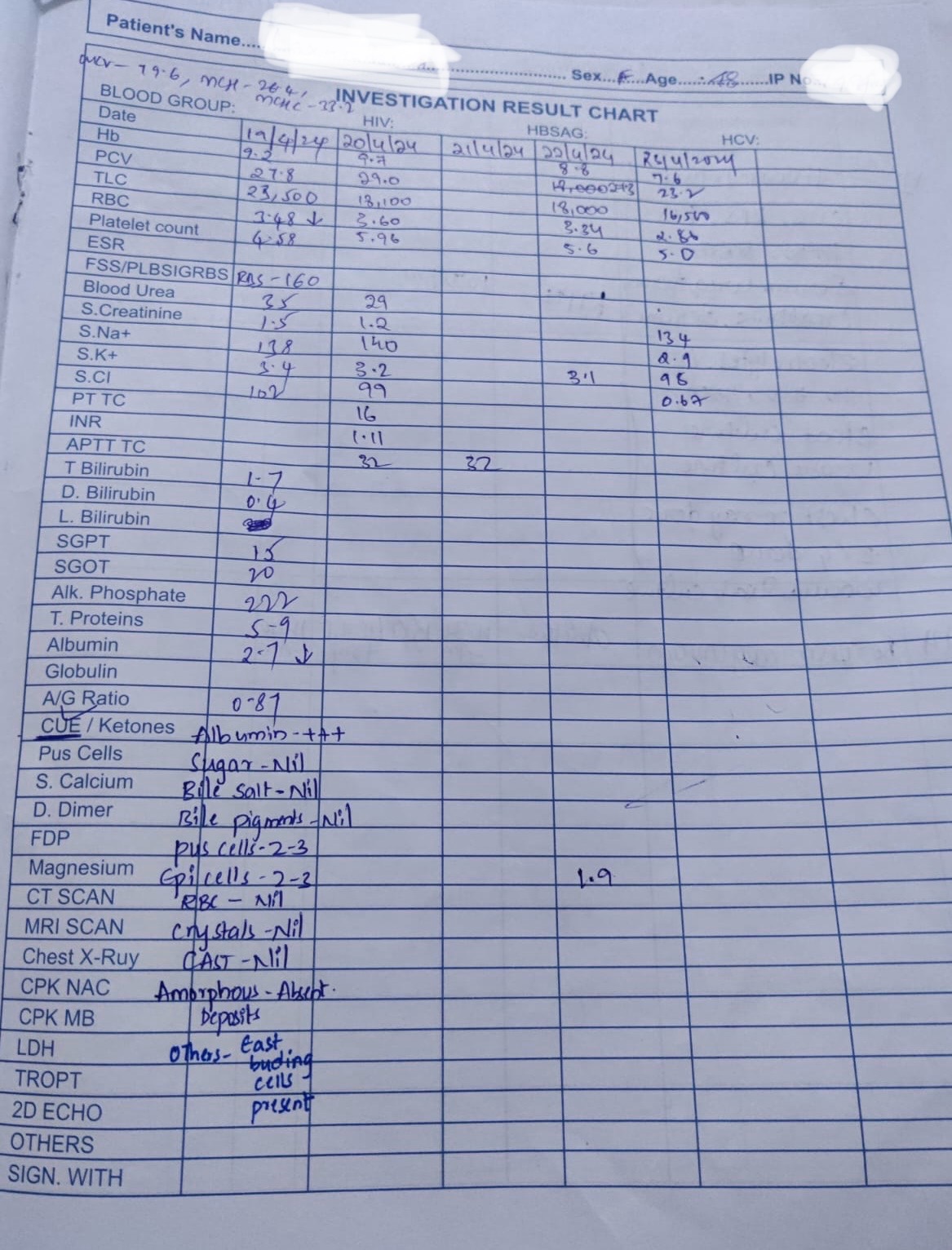
HEMOGRAM: 19/04/24 HB: 9.2 MG/DL
TLC: 23,500 CELLS/CUMM
N/L/E/M/B: 78/17/01/04/00 PCV: 27.8 VOL%
MCV: 79.6 FL
MCH: 26.4 PG
MCHC: 33.2 %
RBC COUNT: 3.48 MILLIONS/CUMM PLATELET COUNT: 4.50 LAKHS/CU.MM SMEAR:NORMOCYTIC NORMOCHROMIC
COMPLETE URINE EXAMINATION (CUE) 19/04/24 COLOUR: PALE YELLOW
APPEARANCE: CLEAR REACTION: ACIDIC SP.GRAVITY: 1.010 ALBUMIN: +++
SUGAR: NIL BILE SALTS: NIL
BILE PIGMENTS: NIL PUS CELLS: 2-3
EPITHELIAL CELLS: 2-3 RED BLOOD CELLS: NIL CRYSTALS: NIL
CASTS: NIL
AMORPHOUS DEPOSITS: ABSENT OTHERS: EAST BUDING CELLS PRESENT
BLOOD UREA 19/04/24: 35 MG/DL SERUM CREATININE: 1.5 MG/DL
SERUM ELECTROLYTES: 19/04/2024
SODIUM: 138 mmol/L
POTASSIUM: 3.4 mmol/L
CHLORIDE: 102 mmol/L CALCIUM IONIZED: 0.96 mmol/L
LIVER FUNCTION TEST (LFT) 19/04/2024
Total Bilurubin: 1.70 mg/dl Direct Bilurubin: 0.40 mg/dl SGOT(AST): 20 IU/L
SGPT(ALT): 15 IU/L
ALKALINE PHOSPHATASE: 222 IU/L TOTAL PROTEINS: 5.9 gm/dl
ALBUMIN: 2.7 gm/dl
A/G RATIO: 0.87
URINE FOR KETONE BODIES 20/04/2024: NEGATIVE BLOOD LACTATE 20/04/2024 : 20 MG/DL
PERIPHERAL SMEAR 20/04/2024:
RBC: NORMOCYTIC NORMOCHROMIC WBC: COUNTS INCREASED ON SMEAR
PLATELET: COUNTS INCREASED ON SMEAR
URINE PROTEIN/CREATININE RATIO 20/04/2024 : SPOT URINE PROTEIN: 15.0 MG/DL
SPOT URINE CREATININE: 14.7MG/DL RATIO: 1.02
24 HOURS CREATININE(URINE) 20/04/2024 : 0.46 G/DAY APTT TEST 20/04/2024 : 32 SECONDS
BLOOD UREA 20/04/24 : 29 MG/DL PROTHROMBIN TIME 20/04/2024 : 16 SEC INR 20/04/2024 : 1.11
HEMOGRAM: 20/04/24 HB: 9.7 MG/DL
TLC: 18,100 CELLS/CUMM
N/L/E/M/B: 71/24/01/04/00 PCV: 29.0 VOL%
MCV: 80.4 FL
MCH: 26.8 PG
MCHC: 33.3 %
RBC COUNT: 3.60 MILLIONS/CUMM PLATELET COUNT: 5.96 LAKHS/CU.MM SMEAR:NORMOCYTIC NORMOCHROMIC
SERUM CREATININE 20/04/24 : 1.2 MG/DL
SERUM ELECTROLYTES: 20/04/24
SODIUM: 140 mmol/L
POTASSIUM: 3.2 mmol/L
CHLORIDE: 99 mmol/L CALCIUM IONIZED: 1.0mmol/L
URINARY PROTEINS (24 HOURS) 20/04/24 : 24 HOURS URINARY PROTEIN: 38.7 MG/DAY
24 HOURS URINE VOLUME: 2,600
URINE PROTEIN/CREATININE RATIO 20/04/2024 : SPOT URINE PROTEIN: 10.0 MG/DL
SPOT URINE CREATININE: 16.0 MG/DL RATIO: 0.6
HEMOGRAM: 22/04/24 HB: 8.8 MG/DL
TLC: 18,000 CELLS/CUMM
N/L/E/M/B: 71/24/01/04/00 PCV: 27.3 VOL%
MCV: 81.7 FL
MCH: 26.2 PG
MCHC: 32.1 %
RBC COUNT: 3.34 MILLIONS/CU.MM PLATELET COUNT: 5.96 LAKHS/CU.MM SMEAR: NORMOCYTIC NORMOCHROMIC
SERUM MAGNESIUM 22/04/2024 : 1.9 MG/DL SERUM POTASSIUM 22/04/2024 : 3.1 MG/DL
HEMOGRAM: 22/04/24 HB: 7.6 MG/DL
TLC: 16,500 CELLS/CUMM
N/L/E/M/B: 70/25/00/05/00 PCV: 23.2 VOL%
MCV: 81.1 FL
MCH: 26.7 PG
MCHC: 33.0 %
RBC COUNT: 2.86 MILLIONS/CU.MM PLATELET COUNT: 5.0 LAKHS/CU.MM SMEAR: NORMOCYTIC NORMOCHROMIC
SERUM ELECTROLYTES: 22/04/24
SODIUM: 131 mmol/L
POTASSIUM: 3.0 mmol/L
CHLORIDE: 105 mmol/L CALCIUM IONIZED: 1.02 mmol/L
SERUM IRON 23/04/2024 : 44 UG/DL
HEMOGRAM: 23/04/24 HB: 7.6 MG/DL
TLC: 16,500 CELLS/CUMM
N/L/E/M/B: 70/25/00/05/00 PCV: 23.2 VOL%
MCV: 81.1 FL
MCH: 26.7 PG
MCHC: 33.0 %
RBC COUNT: 2.86 MILLIONS/CU.MM PLATELET COUNT: 5.0 LAKHS/CU.MM SMEAR: NORMOCYTIC NORMOCHROMIC
SERUM ELECTROLYTES: 24/04/24
SODIUM: 131 mmol/L
POTASSIUM: 3.0 mmol/L
CHLORIDE: 105 mmol/L CALCIUM IONIZED: 1.02 mmol/L
SERUM ALBUMIN 24/02/2024: 2.48 G/DL
BLOOD GROUPING AND RH TYPING : B POSITIVE
HEMOGRAM: 26/04/24 HB: 10.3 MG/DL
TLC: 15,500 CELLS/CUMM
N/L/E/M/B: 71/22/01/06/00 PCV: 31.7 VOL%
MCV: 85.2 FL
MCH: 27.7 PG
MCHC: 32.5 %
RBC COUNT: 3.72 MILLIONS/CU.MM PLATELET COUNT: 5.6 LAKHS/CU.MM
SMEAR: NORMOCYTIC NORMOCHROMIC ANEMIA WITH LEUCOCYTOSIS AND THROMBOCYTOSIS
RFT 26/04/2024:
UREA: 21 mg/dl
CREATININE: 1.1 mg/dl URIC ACID: 2.0 mmol/L CALCIUM: 10.0 mg/dl
PHOSPHOROUS: 2.5 mg/dl
SODIUM: 138 mmol/L
CHLORIDE: 98 mmol/L
HEMOGRAM: 27/04/24 HB: 10.0 MG/DL
TLC: 15,100 CELLS/CUMM
N/L/E/M/B: 66/24/02/08/00 PCV: 30.3 VOL%
MCV: 84.4 FL
MCH: 27.9 PG
MCHC: 33.0 %
RBC COUNT: 3.59 MILLIONS/CU.MM
PLATELET COUNT: 5.2 LAKHS/CU.MM
SMEAR: NORMOCYTIC NORMOCHROMIC ANEMIA WITH LEUCOCYTOSIS AND THROMBOCYTOSIS
SERUM BILIRUBIN TOTAL AND DIRECT 28/04/2024:
Total Bilurubin: 0.82 mg/dl Direct Bilurubin: 0.20 mg/dl
SERUM ELECTROLYTES: 28/04/24
SODIUM: 136 mmol/L
CHLORIDE: 104 mmol/L CALCIUM IONIZED: 1.16 mmol/L
HEMOGRAM: 29/04/24 HB: 10.4 MG/DL
TLC: 12,600 CELLS/CUMM
N/L/E/M/B: 65/26/02/07/00 PCV: 32.6 VOL%
MCV: 82.8 FL
MCH: 26.4 PG
MCHC: 31.9 %
RBC COUNT: 3.93 MILLIONS/CU.MM PLATELET COUNT: 5.2 LAKHS/CU.MM
SMEAR: NORMOCYTIC NORMOCHROMIC ANEMIA WITH LEUCOCYTOSIS AND THROMBOCYTOSIS
SERUM POTASSIUM 29/04/2024 : 4.8 mmol/L
Treatment Given(Enter only Generic Name)
IV FLUIDS NS
INJ.PIPTAZ 4.5 GM/IV/TID
INJ.CLINDAMYCIN 600 MG/IV/BD
INJ.PAN 40 MG/IV/OD AT 8 AM
INJ.HUMAN ACTRAPID INSULIN S/C TID PRE-MEAL ACCORDING TO GRBS
INJ.NPH S/C BD PRE-MEAL ACCORDING TO GRBS
SYP.POTKLOR 15ML PO/BD IN A GLASS OF WATER (I/V/O HYPOKALEMIA )
AMBULATION AND POSITION CHANGE
REGULAR DRESSING OF LEFT FOOT
BP,PR,RR,SPO2 MONITORING 2ND HOURLY
Advice at Discharge
INJ.HUMAN ACTRAPID INSULIN S/C TID PRE-MEAL 12u---10u---6u ( 8 AM,1 PM,8 PM)
INJ.NPH S/C BD PRE-MEAL 10u---0---6u (8 AM, 8 PM)
HOME MONITORING OF GRBS ( PRE MEAL) 8 AM - 1PM - 8 PM)
TAB MVT PO OD
DEBRIDASE OINTMENT FOR LA
Follow Up
REVIEW TO GENERAL SURGERY OPD FOR REGULAR DRESSINGS ON ALTERNATE DAYS. ( DR PRADEEP (GENERAL SURGERY PG) - 95152 28539)
REVIEW TO GENERAL MEDICINE OPD ON FRIDAY .
When to Obtain Urgent Care
IN CASE OF ANY EMERGENCY IMMEDIATELY CONTACT YOUR CONSULTANT DOCTOR OR ATTEND EMERGENCY DEPARTMENT.
Preventive Care
AVOID SELF MEDICATION WITHOUT DOCTORS ADVICE,DONOT MISS MEDICATIONS. In case
of Emergency or to speak to your treating FACULTY or For Appointments, Please Contact: 08682279999 For Treatment Enquiries Patient/Attendent Declaration : - The medicines prescribed and the advice regarding preventive aspects of care ,when and how to obtain urgent care have been explained to me in my own language
SIGNATURE OF PATIENT /ATTENDER SIGNATURE OF PG/
SIGNATURE OF ADMINISTRATOR SIGNATURE OF FACULTY
Discharge Date Date: 29/04/2024 Ward: AMC
Unit: V
Food Plates :